
- Madeline Marshall OMS-III – Edward Via College of Osteopathic Medicine Virginia
- Everett Wilson D.O. – Carilion Clinic Family Medicine Residency
- Christopher John M.D. – Carilion Clinic Department of Orthopedic Surgery
Abstract
Introduction
Focal Periphyseal Edema (FOPE) Zones are a rare MRI finding in pediatric patients. Continued uncertainty around the etiology and future impact of FOPE Zones are still being discussed in current literature.
Case Presentation
A 14-year-old male football player presented with three weeks of vague but worsening left knee pain and a non-specific physical exam. Following unremarkable radiographs, MRI imaging was performed and resulted in a diagnosis of Focal Periphyseal Edema (FOPE) Zone of the left tibia. Conservative treatment of temporary cessation of athletics resulted in resolution of symptoms and allowed return to normal activity with no limitations.
Discussion: This case displays a male athlete which may contribute further to the epidemiologic understanding of FOPE zones. While the cohesive body of research on FOPE is still relatively small, the previously proposed sex difference may equilibrate as more data becomes available, such as in this case of a young male athlete. While this case adds data to the growing literature of FOPE Zones, it also brings about additional questions regarding the assessment and management of knee pain in adolescents.
Conclusion
This case provides insight into the workup, diagnosis, and management of FOPE zones from symptom onset through symptom resolution and provides valuable information to the small existing body of literature on the topic.
Keywords
bone edema, FOPE Zone, growth plate, pediatric knee pain, pediatrics
Introduction
Focal Periphyseal Edema, also known as FOPE Zones, was first described in medical literature in 2011. This finding is described as a benign MRI finding in adolescents. Controversy over the etiology of FOPE is still debated as more research on the topic is currently being published. While the cause of FOPE is still undetermined, there are theories for the etiology of this diagnosis. Today, the body of literature on FOPE is still scant, and as research is continually published on this topic, the etiology and future impact of FOPE Zones may hopefully be determined.
The exact mechanism of focal periphyseal edema is still unknown, but it is postulated that it may be due to growth plate closure. Bones are extremely vascular parts of human physiology. It has been noted that in bones which undergo endochondral ossification, such as long bones like the femur & tibia, vascularity is essential for proper growth plate morphogenesis(1). There is an increase in vascularity in the areas of the epiphysis which may produce small vascular bleeding(2). The bleeding from this area is suspected to create an MRI pattern of edema(2). While this may be a normal process of morphogenesis, bone marrow edema can also be associated with bleeding from trauma or interstitial extracellular fluid leak into the bone marrow(3).
The typical progression of a FOPE Zone diagnosis occurs after a patient presents with or without known injury. Patients who are evaluated for knee pain and find a FOPE Zone incidentally may have some other identifiable cause of their symptoms. In the cases of symptomatic FOPE zones with no other findings, the symptoms may be attributed to the FOPE Zone itself. On literature review, there are no cases of asymptomatic incidental findings of a FOPE Zone. Studies discussing FOPE Zones note a common progression of a patient presenting with pain, having normal radiographs, then having MRI imaging diagnosing the FOPE Zone. The lack of asymptomatic FOPE cases may be attributed to a lack of MRI imaging in patients without pain. While it is thought that FOPE is a normal occurrence, the lack of asymptomatic cases in current literature have caused debate on the true etiology of this diagnosis(4). While FOPE Zones may be a normal process of physeal closure, it would be difficult to determine if this were the sole cause without the presence of this finding in asymptomatic cases.
In the first description of FOPE Zones in 2011, there were no conclusions made about the incidence difference between sexes. However, in this study, seven out of the twelve patients discussed were female(5). In a more recent study comparing 56 patients, a female predominance of 59% to 41% males was noted(6). Again in 2015, a study comparing three cases of FOPE, which were all female, suggested a higher incidence in females(7). Despite this female prominence across limited studies, there is no conclusive research on sex predilection for this diagnosis.
Prompt diagnosis and treatment is recommended to prevent any possible long-term consequences for pathologies involving the physeal plate. Due to FOPE Zones first being described in 2011, the research focused on the long-term effects of this finding is scant. The theory that FOPE zones are benign and associated with normal physiologic growth has led to little follow-up and investigation after resolution of symptoms. In 2018, the first report describing a two year follow up of FOPE Zones in three patients showed no symptoms or limb discrepancies after completion of conservative treatment and observation(8). This study is reassuring for the proposed physiologic nature of this diagnosis and supports the idea that conservative treatment is often appropriate. With this, repeat imaging and surgical intervention are not routinely indicated for the treatment protocol(9). With this objective in mind, discontinuing unnecessary testing and treatment will hopefully result in more cost effective and efficient care(9). Conservative treatment, including supportive care and rest from athletic activity, is considered an appropriate treatment of FOPE Zones.
Case Description
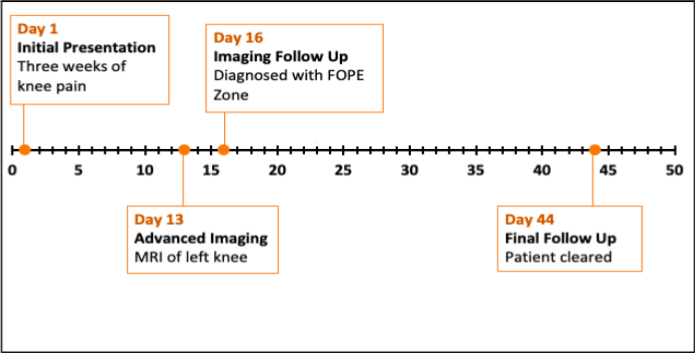
This case follows a 44-day timeline, with initial evaluation starting on day one and last follow up on day 44 (Figure A). The patient, a 14-year-old male presented to the Orthopedic Surgery clinic with three weeks of worsening left knee pain. The patient related the onset of pain with the start of football practice. The pain is described as a dull ache radiating throughout the knee, with localization to the anterior aspect of the knee. A year prior, he had a hyperextension injury to the knee while playing football. Between the previous injury and his pain at initial presentation, he reported mild intermittent knee pain but denied any severe pain. However, on primary assessment, the patient’s symptoms had worsened to limping with walking secondary to the pain. The patient reported his pain was worse with stretching and plyometric exercises. The patient has no previous medical conditions or surgeries.
On exam at initial presentation, there was tenderness to palpation on the left medial tibial plateau. There was no limb malalignment, no pain with patellar compression, and no edema. The knee was neurovascularly intact. Mcmurray’s test was equivocal, and gait was antalgic. Ligament exam was unremarkable, and range of motion was preserved. Full passive range of motion of the hip without pain was noted. Three view X-ray imaging, lateral sunrise, and standing AP of the left knee was unremarkable and showed no fracture, dislocation, or degenerative changes.
Given normal imaging yet continued pain, the decision was made to pursue further diagnostic testing with a left knee MRI. In the interim, the patient was advised against playing football, and against any strenuous lower extremity activity including squats, deadlifts, or any impact training, with no limitations on upper body training.
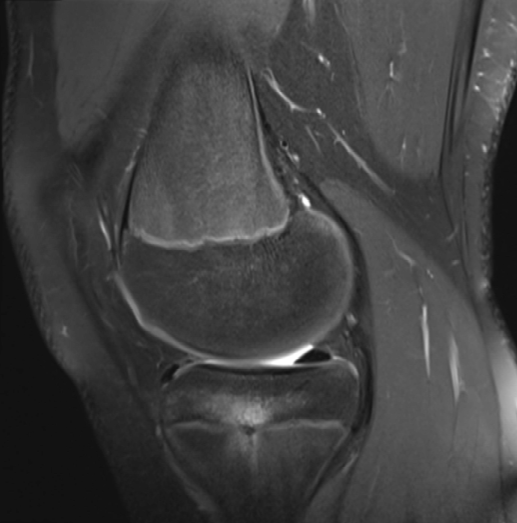
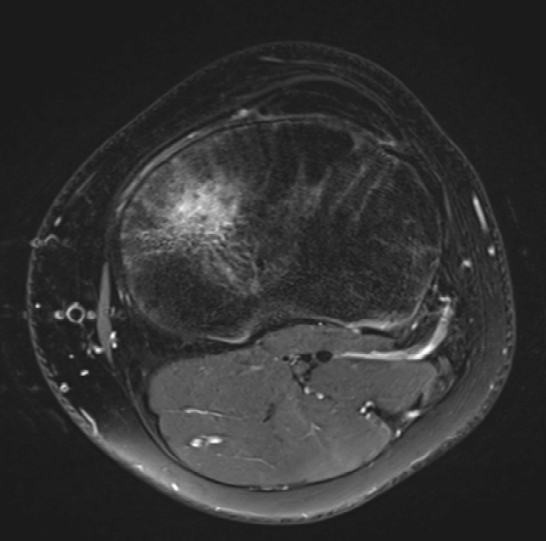
On day 13 of the patient’s 44-day care timeline, the patient had advanced imaging performed. MRI of the left knee showed the left tibia zone of periphyseal edema (Figure B and Figure C).
On day 16 the patient returned for secondary assessment and review of imaging. On assessment, the patient continued having medial knee pain despite cessation from athletics. The patient’s physical exam was unchanged from the initial visit, and MRI findings were discussed with the patient and his mother. After consultation and discussion with pediatric orthopedics, there were concerns for early growth plate closure, and conservative treatment with cessation of athletics for another 4 weeks was recommended. Additionally, the patient was advised to start supplementing vitamin D3 and calcium.
On day 44 of the patient’s care timeline, he returned to clinic with complete resolution of left knee pain. Examination was negative for pain over the medial tibial plateau, negative for general limb malalignment with normal posture, and negative for edema. Ligament exam was unchanged without any signs of ligamentous injury or damage. Range of motion testing was intact, he was able to perform a deep squat, and could squat jump without pain. He was able to ambulate without pain and reported light running on the sidelines at football practice without pain during or after.
In the final presentation, the patient was tolerating activity without any pain. Based on improvement, there was no indication for further imaging. The patient was cleared to return to activity with no limitations. After four weeks of conservative treatment focused at limiting activity the patient was asymptomatic and healed. He was ready to return to activities with no limitations.
Results
Figure A. Timeline of care.
Figure B. Sagittal T2 weighted MRI showing area of focal periphyseal edema surrounding epiphyseal plate of left tibia.
Figure C. Axial T2 weighted MRI showing area of focal periphyseal edema surrounding epiphyseal plate of left tibia.
Discussion
Involvement of the physis raised concern for premature physeal closure. In this case, pediatric orthopedics were consulted and advised prompt cessation of athletics for fear of premature physeal closure. Conservative treatment with cessation of athletics and activities with high impact was sufficient for treatment and resolution of symptoms without invasive treatment or repeat imaging. This illustrates the importance of prompt diagnosis and appropriate treatment of the rare finding of FOPE zone to optimize patient outcomes.
In current literature, there are some studies reporting a higher incidence of FOPE in females when compared to males. This case shows a male athlete which may contribute further to the epidemiologic understanding of FOPE zones. While the cohesive body of research on FOPE is still relatively small, the previously proposed sex difference may equilibrate as more data becomes available, such as in this case of a young male athlete.
In this case, the patient was a known athlete who participated in a contact sport. He also had a history of a hyperextension injury one year prior. Perhaps this, plus the natural process of endochondral ossification, led to the patient’s pain. This case supports the theory that injury may play a more prominent role in the development of FOPE Zones than previously thought, and previous injury should be considered in the management of patient found to have FOPE Zones.
While this case adds data to the growing literature of FOPE Zones, it brings about additional questions regarding the assessment and management of knee pain in adolescents. For example, it is interesting to consider how many diagnoses of Osgood-Schlatter or “growing pains” are FOPE zones. Additionally, once FOPE Zones are diagnosed and found, the current sparse guidelines do not recommend repeat imaging. However, perhaps there are times when repeat imaging is warranted, especially in more active adolescents eager to get back to sport. Also, should practitioners rely on imaging showing resolution, or symptom improvement. The proposed theories of natural physiologic process versus altered mechanics and injury indicate the importance of further research on this topic, as there is clearly much more to ascertain in the assessment and management of FOPE Zones.
Summary
This case displays the progression from diagnosis of Focal Periphyseal Edema to treatment and resolution of symptoms. It helps add valuable data to the growing investigation of this rare MRI finding. While FOPE Zones were originally thought to be a natural process associated with growth plate closure, the controversy over the etiology leads to continued debate on the topic.
Conclusion
This case displays an effective diagnosis and treatment of FOPE Zone in an adolescent male patient and helps broaden the scope of existing research on this rare MRI finding. It supports the theory that injury may play a role in development of focal periphyseal edema, and adds data to the epidemiologic aspect of this diagnosis. It also further supports the theory that conservative management of FOPE Zones is often appropriate.
References
- Filipowska J, Tomaszewski KA, Niedźwiedzki Ł, Walocha JA, Niedźwiedzki T. The role of vasculature in bone development, regeneration and proper systemic functioning. Angiogenesis. 2017 Aug;20(3):291-302. doi: 10.1007/s10456-017-9541-1.
- Zbojniewicz AM, Laor T. Focal Periphyseal Edema (FOPE) zone on MRI of the adolescent knee: a potentially painful manifestation of physiologic physeal fusion?. AJR Am J Roentgenol. 2011;197 (4): 998-1004.
- Hayes CW, Conway WF, Daniel WW. MR imaging of bone marrow edema pattern: transient osteoporosis, transient bone marrow edema syndrome, or osteonecrosis. Radiographics. 1993 Sep;13(5):1001-11; discussion 1012. doi: 10.1148/radiographics.13.5.8210586.
- Thomas Bochmann, Richard Forrester, Jon Smith, Case report: imaging the clinical course of FOPE—a cause of adolescent knee pain, Journal of Surgical Case Reports, Volume 2016, Issue 11, November 2016, rjw178, https://doi.org/10.1093/jscr/rjw178.
- Shim KS. Pubertal growth and epiphyseal fusion. Ann Pediatr Endocrinol Metab. 2015 Mar;20(1):8-12. doi: 10.6065/apem.2015.20.1.8.
- Wu M, Bixby S, Kramer DE, Heyworth BE. Focal Periphyseal Edema (FOPE): A Newly Reported Cause of Knee Pain in Adolescent Athletes. Orthopaedic Journal of Sports Medicine. 2018. doi:10.1177/2325967118S00135.
- Nicholas Beckmann, Susanna Spence, “Unusual Presentations of Focal Periphyseal Edema Zones: A Report of Bilateral Symmetric Presentation and Partial Physeal Closure”, Case Reports in Radiology, vol. 2015, Article ID 465018, 8 pages, 2015. https://doi.org/10.1155/2015/465018.
- Ueyama, Hideki Kitano, Toshio Nakagawa, Keisuke; Aono, Masanari. Clinical experiences of focal periphyseal edema zones in adolescent knees: case reports. Journal of Pediatric Orthopaedics B 27(1):p 26-30, January 2018. | DOI: 10.1097/BPB.0000000000000388.
- Giles E, Nicholson A, Sharkey MS, Carter CW. Focal Periphyseal Edema: Are We Overtreating Physiologic Adolescent Knee Pain? 2018 16;2(4):e047. doi: 10.5435/JAAOSGlobal-D-17-00047.
Required Disclosures and Declaration
Copyright Information: No Copyright Information Added
IRB Approval Information: Not applicable
Disclosure Information: No known conflicts of interest

{kind=link}
{kind=link}
{kind=link}